A scientific research institute that has been dedicated to basic, discovery science for several decades is launching a new project focused on human brain health.
The Brain Health Accelerator, which the Allen Institute announced today, aims to create genetic medicines for five neurodegenerative diseases: Alzheimer’s, Huntington’s and Parkinson’s diseases, Lewy body dementia and ALS. Its aspiration is to test a treatment in people within five years for at least one of these conditions, says Ed Lein, executive director of the project.
“This is an enormously important thing to do,” says Bing Ren, scientific director and CEO at the New York Genome Center, who is not currently involved in the project but hopes to collaborate. The timing of the effort “couldn’t be better,” given the recent slowdown of funding from the U.S. National Institutes of Health.
The 14-year, $400 million project uses the tools and techniques the Allen Institute has helped develop, including single-cell atlases of the human brain and viral vectors designed to deliver gene therapies to specific cell types. Half of the funding comes from the Allen Institute, and the other half includes contributions from the Bezos family, Amazon Web Services, the National Institutes of Health and the nonprofit organization EverythingALS, a press representative of the Allen Institute told The Transmitter.
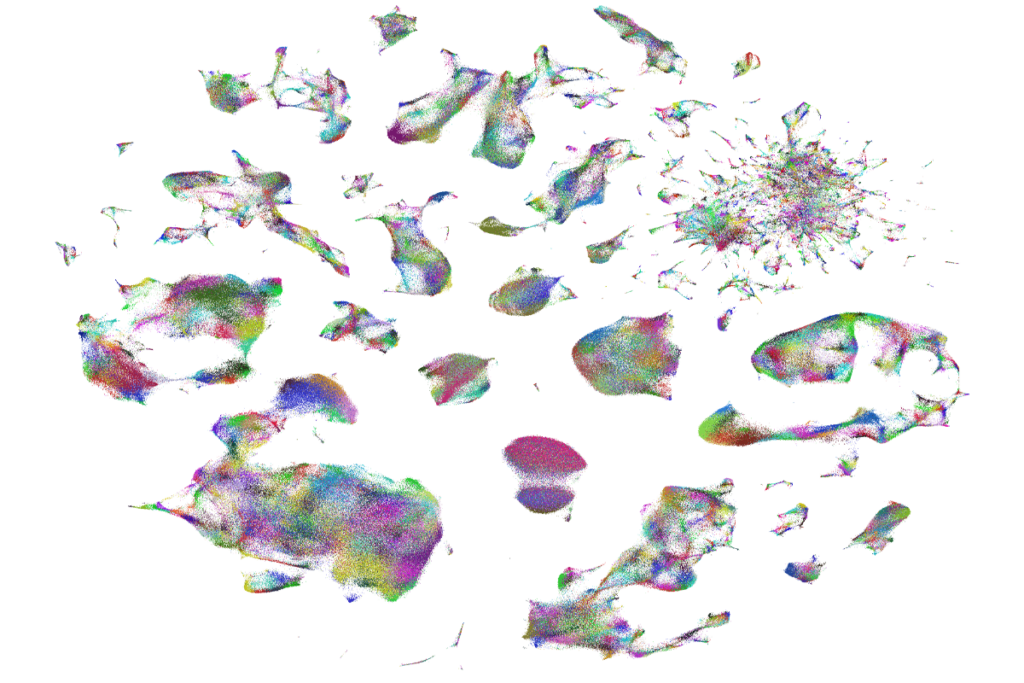
The team plans to use single-cell transcriptomics to understand the baseline biology of each disease, including how it progresses and which cell types and circuits it affects, and then develop genetic medicines that can offset those changes.
“What they’re doing is going to be really quite powerful,” says Walter Koroshetz, former director of the National Institute of Neurological Disorders and Stroke and senior adviser at the Dana Foundation, who is not involved in the project.
Probing the RNA expression of individual cells has offered fresh insights into disease. For example, in Huntington’s disease, neurons carry a repetition of the DNA triplet CAG but are not harmed until the sequence recurs more than 150 times, a 2025 study reported. “It completely changed how people think about Huntington’s disease,” Koroshetz says. This pattern would have been impossible to spot with bulk sequencing methods because the neurons quickly die after reaching 150 repeats, he adds; you notice it only when you look cell by cell.
And in Alzheimer’s disease, a subtype of inhibitory neurons are the first to die, according to a single-cell atlas project Lein and his colleagues published in 2024.
Scientists have failed to develop effective treatments for neurodegenerative disorders in part because observations in rodent models don’t always translate to people, says John Morrison, distinguished professor of neurology at the University of California, Davis, who is in the process of setting up a collaboration with the Brain Health Accelerator.
“Everything that they are going to do in this initiative will be grounded in the human brain and human brain health, and I think that’s a very, very smart move,” Morrison says.
T
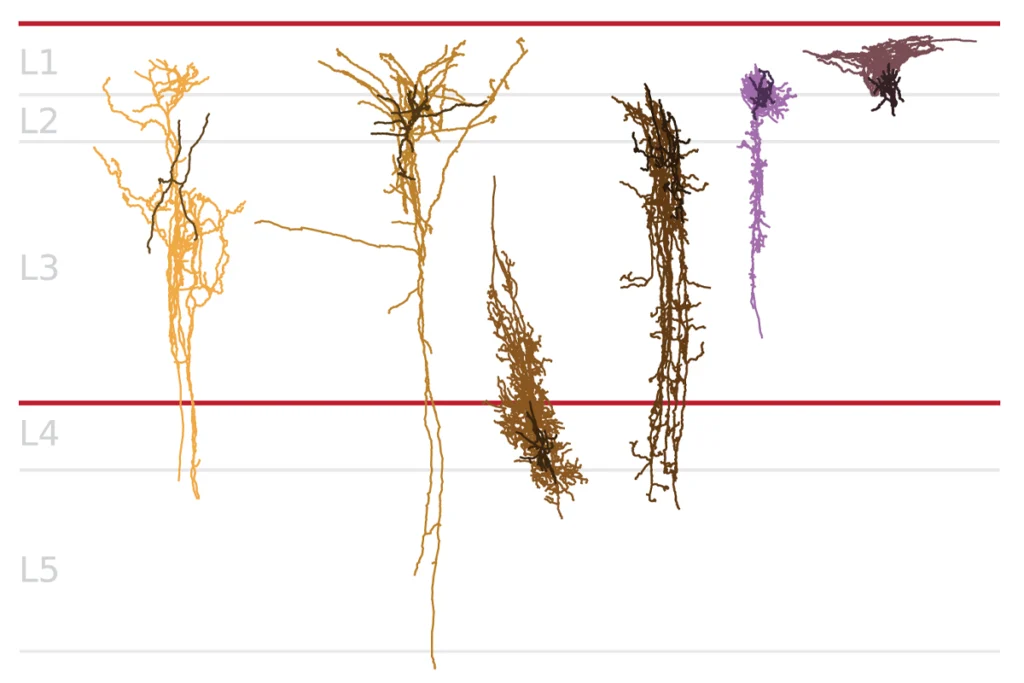
he Allen Institute published a gene expression atlas of the mouse brain in 2006, and later a single-cell resolution version, but creating a similar atlas of the human brain proved to be “really challenging,” Lein says, in part because of the brain’s size and complexity but also because of tissue degradation. He and his colleagues published a first step toward that goal in 2023, thanks to improvements to single-cell sequencing technology and human postmortem brain tissue processing driven by the BRAIN Initiative Cell Census Network.“It’s reached the point where the human studies don’t have to be secondary to model system studies,” Lein says. “We can actually do those right out of the gate and get a ground truth understanding of the actual structure of the human brain and what goes on in disease.”
The gene expression and regulation differences that demarcate different cell types also offer opportunities to target one kind of cell versus another. Adding an enhancer to the expression cassette in a gene therapy can help ensure that a treatment is delivered only to the cells that need it, increasing potency and decreasing off-target effects, Lein says.
That approach proved effective in an experimental gene therapy for Dravet syndrome that provides a replacement copy of the sodium channel gene SCN1A only to interneurons. Dravet model mice that received the treatment had fewer seizures than did those without treatment, and fewer mice died prematurely.
Designing these cell-type-specific treatments for brain diseases is “exactly the right approach,” Morrison says.
The viral vector technology used to deliver gene therapies is still being fine-tuned, though. The high viral load required can cause liver toxicity, adverse immune reactions and even death; last year, a child died after receiving a dose of a gene therapy for the rare disorder syntaxin-binding protein 1 encephalopathy.
Researchers have also struggled to develop viral vectors that pass safely from the bloodstream into the brain. One way to get around this problem is to inject a therapy directly into the affected brain area, Lein says, but that tactic falls short for treatments that need to reach the entire brain.
“If advances are made that really overcome some of these barriers, we will adopt them immediately,” Lein says. “Our technology fits into any viral system.”
The project is intended to be a giant collaboration among many institutions, Lein adds. “These are very complicated efforts, and the problem is just way too big for one place.” Collaborations will be particularly important for the treatment development part of the work, he says, because the Allen Institute has never run a clinical trial.
Although the program is focused on five neurodegenerative diseases for now, the team might expand it to include epilepsies and neurodevelopmental and neuropsychiatric conditions, Lein says. “We’ll see where the program leads and where we could have the biggest impact.”